SAMARTH PHARMA
Its necessary for surgeries to be done successfully & for operations to run smoothly & without pain, that’s why studying them extensively is important so that to be able to go further more later on in discovering new agents with lower side effects & more efficiency , & they are (anaesthetics) divided into 2 major types which are as the followingA) Local Anaesthetics B) General Anaesthetics

Please Press on the picture to enlarge it & read the content clearly

Its necessary for surgeries to be done successfully & for operations to run smoothly & without pain, that’s why studying them extensively is important so that to be able to go further more later on in discovering new agents with lower side effects & more efficiency , & they are (anaesthetics) divided into 2 major types which are as the followingA) Local Anaesthetics B) General Anaesthetics
And in this lecture & the coming parts & episodes of it, I’m going to discuss & revise GENERAL ANESTHETICS from Clinical point of view & from Pharmacological point of view depending basically on hard medical books & references + my personal old university lecture notes
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=
Physiochemical Theories of Anaesthesia
Unlike most of the other drugs in pharmacology, General Anaesthetic agents are not exactly & totally understood from pharmacological mechanism of action point of view until now, since they have different chemical structures & electronic configuration -anaesthetic agents- so they are not belonging to any basic single chemical class, the pharmacological action of general aneasthetics requires basically a specific uniimportant physiochemical properties, those agents lacks an exact RECEPTOR which they work in & they have a low profile in chemical specificity regarding this matter
They appear to act principally on the cells membranes & the theories of anaesthesia focuses on the interactions with the 2 major components of the cell membrane which are the lipids & proteins, That’s why General Anaesthesia Theories would be divided into 2 major sections which are as the followingA) The Lipid TheoryB) The Protein Theory
Note also that there are another theories available in the scientific field but I concentrated on those 2 major ones since they are the basic original theories mentioned in pharmacology references & were taught to us before
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-=
A) THE LIPID THEORY
The Lipid Theory is based on the idea that there is a close correlation between the Anaesthetic Potency & the Lipid Solubility of the agent, & it believes that Narcosis commences (Narcosis means exactly the privation of sense & consiousness due to using a nracotic agent) when any chemically indifferent substances has attained a certain molar concentration in the lipids of the cells, so the agent must be lipid soluble & to reach a specific molar concentration, when those 2 factors occurs, the anaesthetic affect will start also
Now in general and before going deeper into this particular theory, it is well known in the medical field that for a substance in general to be able to pass the cell membranes, it needs to be holding a special percentage of lipid solubility so that to pass the LIPID membranes of the living cells in general, for sure there are other mechanisms of excerting actions on the cells other than being only lipid soluble, but still lipid solubility plays the major role in this reaction & this is why the LIPID THEORY is a logical theory which depends on a basic scientific evidence
The relationship between anaesthetic activity & lipid solubility has been repeatedly confirmed, see the following diagram which shows results obtained in humans where the Minimal Alveolar Concentration (MAC) which is inversely proportional to potency required to produce a lack of response to painful stimulation is plotted against lipid solubility

Please Press on the picture to enlarge it & read the content clearly
It is expressed as oil : water partition coeffiecient (the past diagram shows oil in gas partition & it is the saem concept since I couldn’t find the exact diagram that I want), for a wide range of inhalation anaesthetics, This diagram is called the Overton-Meyer studies & it did not suggest any particular mechanism of action, but it showed a basic interesting correlation which any theory of anaesthetics needs to take in account in general, the oil : water partition should predict the partition into membrane lipids, while the keeping the old agreement that anaethesia make an alteration in the membrane function
Now the right question would be that HOW might the introduction of an inert new substance molecules into the cell membranes causes a full disturbance in those cells & causes a clear functional disturbance & changes? To answer this questions there are different ideas, in which one of them is called "The pressure reversal anaesthesia theory" which indicates that the "Volume Expansion" is the reason of those past mentioned effects, In animals such as newts, they are immobilised by the addition of an anaesthetic agent to the water, then the application of hydrostatic pressure to about 100 atmospheres immediately restores their mobility & the anaesthesia returns as soon as the pressure is lowered
Those results are compatible with the theory that anaesthesia occurs when volume of the lipid phase is expanded by about 0.4% as a result of the intrusion of anaesthetic molecules, Pressure is though to act simply by opposing this volume expansion, further work decreased also the doubt regarding this point of view
Another theory involves the increase in membrane fluidity due to the disorder that occurs in the packing array of membrane phospholipids, all the physiochemical measurments confirms that this happens, so, relatively high concentrations of the anaesthetic agents is needed & the affects are small by comparison with those of a modest (<1 degree C) rise in temperature, so also the relation directly between this theory & the pharmacological action is not exactly clear
=-=-=-=-=-=-=-=-=-=-=-=-=-=-=-
B) THE PROTEIN THEORY
Anaesthetics can bind to proteins as well as lipids, studies done on some kind of "enzymes" which means some kinds of proteins showed that there is a parallel relation between the action of enzyme inhibition & the anaesthetic agents functions, there were another evidences of relation between anaesthetic actions and the interaction with the functional membrane proteins, for example ligand-gated ion channels, A lot of anaesthetic agents at a concentration reached to cause anaesthesia had shown to inhibit the functions of excitatory receptors "like ionotropic glutamate acetylcholine or 5-HT receptors" as well as enhancing the inhibitory receptors functions "like GABA A & Glycine", the studies after that done on genetically engineered receptors showed that the effects depends on the presence of a particular domains in the receptor protein, which comprise specific "Modulatory sites"throug which the anaesthetic drugs exerts their effects on channel functions, there must be further studies done to clearify this effect and the past mentioned points, especially those experiments done on mice
From holding a moderate middle level of understanding both theories the lipid & the protein theory is athe basic view that the anaesthetics concentration at the lipid-protein interface within the cells membranes is important for the pharmacological action to occur & we have to keep in mind that most proteins have different or multi-functional reactions which will include more than one theory as a
In the past episode we spoke about anaesthesia in general, & we said that anaesthesia is a great discovery in medical studies since it help the surgical painful procedures to go on smoothly & without pain. At the same time we said that anaesthetic agents doesn’t follow a specific chemical category, neither they follow any specific mechanism of action, since there is a wide variety of agents which are used & different mechanisms combined at the same time to produce the pharmacological effects
In this part we’ll go more deeper discussing anaesthetic agents & their effects on the Nervous System in a more deeper & scientific manners
THE EFFECTS OF ANAESTHETICS ON THE NERVOUS SYSTEM
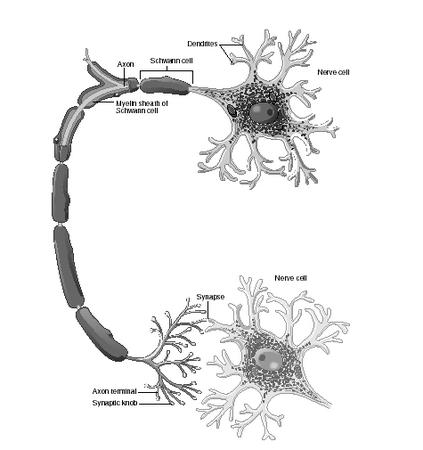
At the beginning & before discussing this topic, it is important to remember from the last lecture that there are 2 basic theories of anaesthetics actions which are the protein theory & the lipid theory, Now, whatever was the theory, at the end there is an activity of those anaesthetic agents which is produced on the cellular levels normally, which acts basically on the synaptic transmission & as we all now, the synaptic transmission is the basic process in which the neurotransmiters will be sent from one nervous axon to the other & through this mechanism we’ll feel the pain coming from the peripheral nervous system & reaching the brain to be translated as pain, so anaesthetics works by interupting this transmission in a way or other which helps reducing or cancelling the sensation of the pain at a particular time
So the effects on the axonal conduction process is considered to be a critical part in the practice of anaesthesia on patients, so the inhibition of this synaptic conduction process can be acheived in different mechanisms including the following
A) By decreasing the neurotransmitter release processB) By the inhibition of the action of the neurotransmitterC) By the reduction of the excitibility of the postsynaptic cell
Through the past mentioned mechanisms, the reduction in the transmitter release & \ or the reduction in the excitibility of the postsynaptic cell are the most studied kinds & the most acceptable ways on actual clinical studies
For example, the reduction of Acetylcholine release was shown & proved in some peripheral nerves, at the same time, a decrease in the postsynaptic sensitivity had been shown in both central & peripheral nervous system studies & this decrease in the sensitivity was due to the inhibition process of the ligan-gated ion channels there, & this last process "the decrease in the postsynaptic sensitivity" was shown for example with BARBITURATES, in which they enhanced the low sensitivity process in these areas & at the same time this effect was occuring also with some volatile anaesthetics
Studies also were done to understand the exact region in the brain which was responsible for the anaesthetics action & these studies showed in a way or another that the THALAMIC SENSORY RELAY NUCLEI & THE DEEP LAYER OF THE CORTEX TO WHICH THESE NUCLEI PROJECT were the most sensitive areas working along with the anaesthetics, this area includes the routes taken by the sensory impulses to reach the cortex, so the general idea is presented by inhibiting this transmission & inhibiting the sensory impulses from reaching the cortex through this route, which means at the end that the brain will not receive the impulse & will not generate the feeling of PAIN at the end, another theory which enhance our awareness about the brain function is that anaesthesia even in small concentrations causes a mild AMNESIA effects on the patients, this is due to the interference which happens between the anaesthetic agent & the hippocampal functions & it is known that the hippocampus is the responsible for the short-term memory functions, thats’ why mild experiences with the anaesthesia can’t be exactly & directly remembered by the patient even if with small doses of the anaesthetic agent
And as the anaesthesia dose increase, the brain functions as a whole organ will be effected tissue by tissue, including the motor control & the reflex activities, the respiration & the autonomic regulations, so at the end & while increasing the dose of the anaesthsia, we can’t exactly describe a specific site in which the anaesthetic agent will work on it
BRIEF
Briefly we can say & as a continuing to the past lecture that there are evidences showing & describing the general actions of the anaesthesia, in which it have to be lipid & protein soluble to some extends, it will effects the cell structure & walls & will effect the conduction mechanism in them, through decreasing the release of neurotransmitter & through enhancing the decrease in the sensitivity of the postsynaptic cells, it will exert its’ effects
In smaller doses it will cause amnesia & effect the hippocampal functions & by increasing the dose it will start effecting all the brain as a general whole organ making it more difficult to predict the exact location of its pharmacological actions
TO BE CONTINUED
No comments:
Post a Comment